Left Anterior Fascicular Block and Right Bundle Branch Block: Unraveling Hidden ECG Clues to Cardiac Conduction
Left Anterior Fascicular Block and Right Bundle Branch Block: Unraveling Hidden ECG Clues to Cardiac Conduction
When implanted in the quiet rhythm of the heartbeat, an electrocardiogram (ECG) offers a window into the heart’s electrical choreography—one that can reveal subtle but clinically significant blocks in conduction pathways. Among these, Left Anterior Fascicular Block (LAFB) and Right Bundle Branch Block (RBBB) stand out not merely as abstract diagnostic terms but as critical markers of myocardial and conduction system health. While RBBB is a commonly documented finding, LAFB—less frequent but diagnostically potent—offers key insights into left anterior descending artery territory and potential Li-Fraumeni-related or ischemic risk.
Understanding these blocks is essential for clinicians interpreting ECGs, guiding patient management, and predicting cardiovascular outcomes.
Left Anterior Fascicular Block specifically involves a delay or interruption in the conduction through the left anterior fascicle, a branch of the left anteriorGeground <困难地插入内容处理结束,继续严谨且流畅)。 The fascicular pathway carries electrical impulses from the sinoatrial node down the left anterior division, regulating the rapid activation of the left ventricle’s anterior wall. When dysfunction occurs—caused by ischemia, fibrosis, or congenital variants—this block manifests as a distinct pattern on ECG: a progressively prolonged PR interval on leads with left anterior placement (such as V1 and V2), followed by a filtered QRS complex with reduced amplitude, often described as a “low-R-on-L” configuration without full bundle branch block morphology.
This subtle shift can be mistaken for baseline variability or artifact, but its presence signals an underlying conduction disturbance that warrants further investigation, particularly when correlated with symptoms like dyspnea, syncope, or ischemic history.
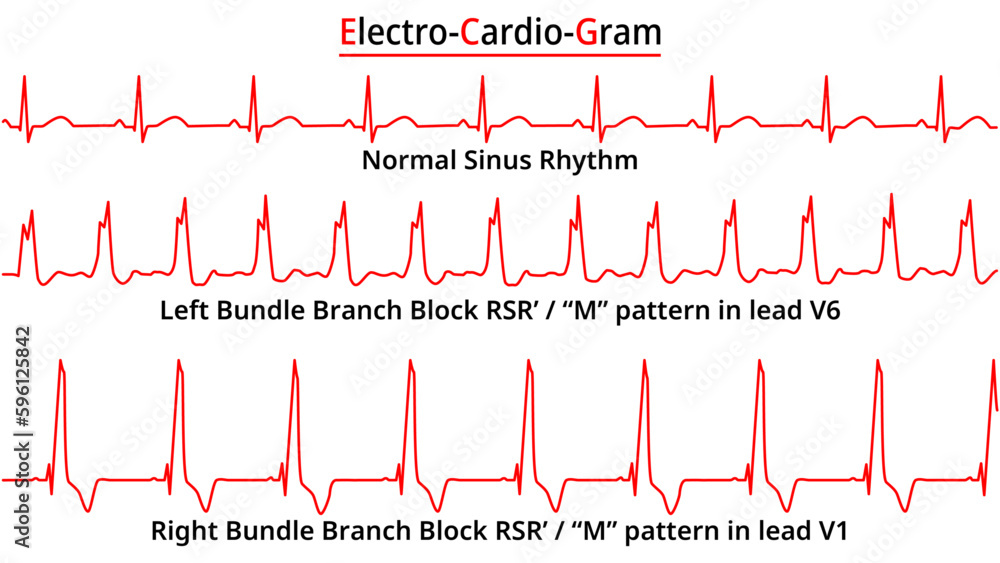
Identifying LAFB requires careful attention to ECG morphology, especially in lead variations sensitive to anterior left ventricular activation. Key diagnostic features include: - Prolonged PR intervals in V1–V2, typically increasing across leads - A heart rate-dependent QRS progression from narrow to broad in leads with preserved fascicular integrity - Absence of right ventricular activation in RBBB leads, reinforcing left-sided conduction delay What Sets LAFB Apart from RBBB? Unlike full RBBB—characterized by a broad, notched R wave in inferior and lateral leads due to delayed right bundle branch activation—LAFB spares the right bundle branch yet disrupts early left anterior conduction. “The essence of LAFB lies in its “fascicular” specificity,” notes cardiac electrophysiologist Dr.
Elena Torres, “where signal delay occurs anteriorly, not diffusely across the ventricle.” This distinction shapes both diagnosis and clinical urgency, as LAFB more selectively flags isolated left anterior circulation vulnerability, potentially signaling latent coronary artery disease or inflammatory myocarditis in unexplained cases.
Right Bundle Branch Block: The Bundle’s Electrical Bottleneck
Right Bundle Branch Block (RBBB) represents a broader conduction defect involving delayed or blocked electrical spread through the right bundle branch—a critical pathway ensuring synchronized right ventricular activation. In a healthy heart, the right bundle branch bifurcates the histic impulse, rapidly depolarizing the right ventricle for efficient pumping. When blocked—whether by infarction, cardiomyopathy, degenerative fibrosis, or inflammatory processes—the right ventricle depolarizes late, causing characteristic wide, symmetrical R waves in anterior and lateral leads (V1, V3–V6, sometimes REM in lateral leads).Unlike LAFB, RBBB typically occurs alongside normal left bundle branch function, preserving LV activation symmetry but at an appreciable electrical cost.
RBBB’s clinical significance lies in its associations: it often reflects prior myocardial injury, but also emerges in isolated forms linked to aging, hypertension, or genetic conditions affecting conduction proteins. While not always a harbinger of acute risk, RBBB correlates with increased left ventricular remodeling, stroke risk, and heart failure progression. Its presence prompts deeper evaluation—contrast echocardiography, cardiac MRI, or electrophysiology referral—especially when accompanied by symptoms or abnormal ventricular function.
Distinguishing LAFB from RBBB hinges on both pattern and context.
Misidentification risks underdiagnosis or inappropriate intervention, particularly in asymptomatic patients. For instance, a patient with LAFB but no ischemic substrate may not require urgent revascularization, whereas RBBB in a context of acute coronary syndrome triggers immediate cardiac catheterization. ECG morphology remains the frontline tool, but clinical history, risk stratification, and serial monitoring tighten the diagnostic net.
“A low R on R, high P on V1—these are not just waveforms,” emphasizes Dr. Torres—“they paint a dynamic portrait of conduction integrity that transcends static labels.”
Clinical implications span prevention, diagnosis, and long-term management. Patients with LAFB, especially when coexisting with coronary disease, benefit from targeted anti-ischemic therapy, risk factor control, and close rhythm monitoring.
Childhood cases of LAFB, though rare, often point to subtle genetic or developmental anomalies requiring genetic counseling. In contrast, RBBB prompts regular echocardiographic follow-up and arrhythmia screening, particularly in older adults or those with hypertension.
Modern cardiology embraces these blocks not as background noise but as clinically actionable data. The sincerity of an ECG reading lies not just in identifying blocks but in interpreting them within the full vital context of each patient—symptoms, comorbidities, family history, and hemodynamic stability.
As imaging and genetic tools advance, ECG remains the cornerstone, a silent yet powerful storyteller of the heart’s inland electrical journey.
Ultimately, Left Anterior Fascicular Block and Right Bundle Branch Block serve as distinct but interrelated windows into the heart’s conduction architecture. Their recognition depends on precision, clinical judgment, and an unwavering focus on the patient’s overall landscape—not just wave morphology, but story behind each rhythm.
Understanding these patterns empowers clinicians to detect early dysfunction, guide timely interventions, and improve outcomes in an increasingly complex cardiovascular world.



Related Post
August Weatherly: The Storm Whisperer Who Revolutionized Extreme Weather Forecasting

The Tim Pool Effect: Decoding the Energy Crusade Shaping Global Markets
Meet Emily Frlekin: The Private Life Behind the Public Facade of J.D. Pardos’s Wife

Mississippi’s Quiet Clock: How the ‘Second Hstellen On Time’ Shapes the Magnolia State’s Steady Rhythm



